|
A Midwestern Doctor from The Forgotten Side of Medicine <amidwesterndoctor@substack.com> |
Sun, Apr 7, 2024 at 5:52 PM |
||||||||||||||||||||
|
Reply-To: A Midwestern Doctor from The Forgotten Side of Medicine <reply+2dcaem&doii8&&1a19949fcf38cf33e0a922451c3d5f13af2663a567693d5e1f56ad6a54032b85@mg1.substack.com> To: fchase@gmail.com |
|||||||||||||||||||||
|
|||||||||||||||||||||
I feel one of the biggest issues in modern medicine is that patients often don’t get the opportunity to establish a genuine relationship with their physician and hence often lack the critical voice which is necessary for a therapeutic doctor-patient relationship.
Because of this, my goal here was always to be able to correspond with everyone who reached out to me (e.g., through comments). Unfortunately, due to the unexpected success of this publication, I don’t have the time to both do that and to write here. For that reason, I decided the best solution was to have monthly open threads where people could ask whatever they wanted on any topic and I would make a point to always reply to them.
In tandem with these open threads, I try to have them tie to a subject that I feel is important to cover, but doesn’t quite merit being the focus of an entire article. For this month’s open thread, I want to focus on the many unappreciated dangers of clothing, how unhealthy clothes adversely affect our lives (often without us realizing) and the ways we’ve identified for over the years to address this.
However, before going into how to have a healthy wardrobe, I had a two loose ends to tie up.
First—One
of my goals with this publication has been to bring attention to local groups
who are doing important work that relates to the themes of this newsletter but
have very little support or awareness of their struggle and are hence in a
David vs. Goliath situation (I’ve always been drawn to supporting the
underdog). This for example is why I’ve tried to expose the reckless lab
altered mosquito experiment the biotech industry is forcing
upon Hawaii.
Most recently, I published an investigation into
a biolab the NIH is spending millions to create in Fort Collins CO which is
meant to be the national center for experimenting with viruses in bats. Since
that lab has a lot of parallels to Wuhan (e.g., the university hosting it has a
long history of lab accidents and its staff have close ties to both the funders
and employees of the Wuhan bat lab) people in the community are understandably
concerned about it. Sadly, Colorado’s government (which stands to make a lot
from the project) has stonewalled them and the local community is in a very
similar situation to the people in Maui trying to stop the
mosquitos.
Immediately after I published the article, something very strange happened—for
some reason their website got taken down. Since my goal for the article was to
rally support for what they were doing, I wanted to instead provide a link to their Facebook
group for those who wish to be involved.
Note:
additionally, after I wrote that article, Meryl Nass told me that when I
discussed the flurry of vaccine mandates that were passed in 2019, CT also lost the option for a religious
exemption. I missed this critically important point because it was passed in
2021 and hence did not appear on the 2019 lists.
Second—in the article I recently wrote about the importance of zeta potential, a few important points were omitted from it I later added in (i.e., that far more subtle cranial nerve deficits an experienced clinician can detect frequently occur after vaccination and that one of the major issues with the mRNA vaccines was that some of them had defective lipid nanoparticles which adversely affected the physiologic zeta potential). Additionally, one of the most common questions I received from there was where our protocols for treating zeta potential could be viewed. They are covered within this article:
How to Improve Zeta Potential and Liquid Crystalline Water Inside the Body
|
||||||
|

|
|
||
|
Additionally, in the February’s open thread, I surveyed which future article topics had the most interest and I am presently working on one about Dermatology’s War Against the Sun (and the skin cancer racket) since it was one of the most requested topics.
A Chance Plane Ride
Years ago, a friend of mine was seated on a plane next to a chief executive of a major American chemical company that was notorious for polluting the environment and sickening large numbers of Americans with its products. After building up a friendly rapport, my friend asked the executive what he considered to be the most important piece of advice he had to share. The executive immediately responded:
Always wash new clothes before you put them on.
I’ve never forgotten that story, and over time my patients have helped me to appreciate just how many nasty chemicals end up on our clothing most of us never notice.
Canaries in the Coal Mine
Birds
tend to be much more sensitive to environmental toxins than humans (e.g., I’ve
read numerous stories of birds dying while in the vicinity of someone cooking
with a teflon pan). This principle in turn was utilized by coal miners who were
always at risk of a lethal toxic gas buildup (particularly of carbon monoxide)
occurring in the mines. Since carbon monoxide is odorless, they would bring canaries with them and if the canaries
suddenly died, they immediately got out as they knew they eventually would too.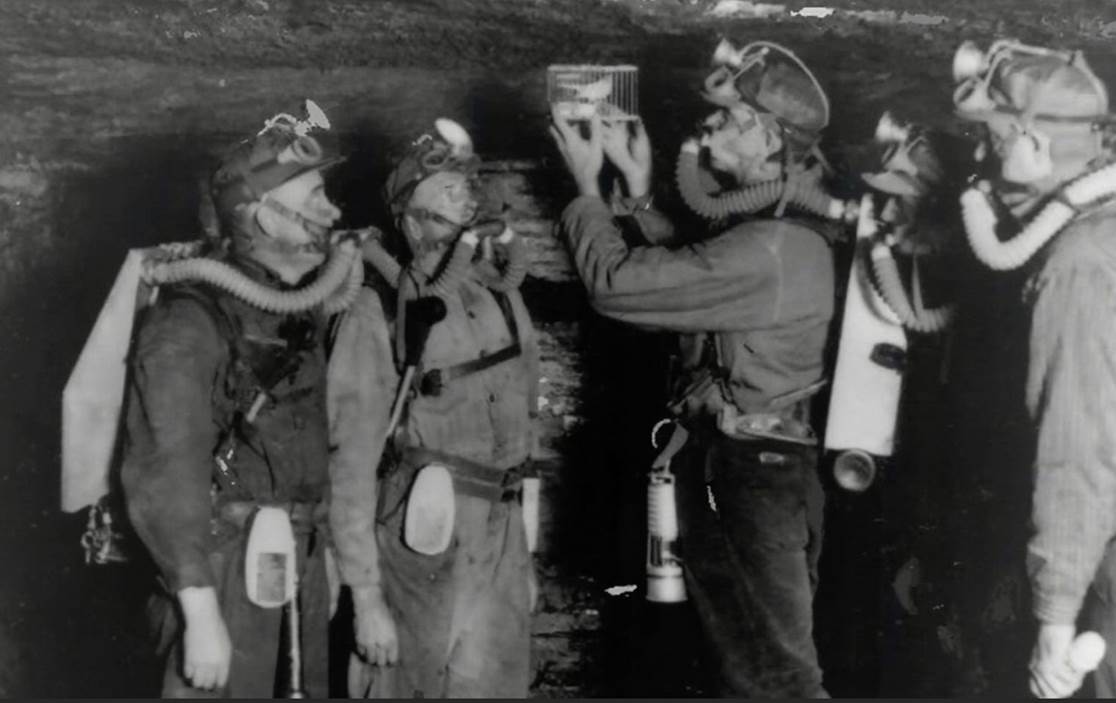
One of the fundamental principles in statistics is that variable phenomena tend to distribute on a bell curve, with the average value (e.g., adult American men being 5’9—which is a bit above the global average) being by far the most common, while values become exponentially rarer as they move further away from that mean (e.g., only 15% of adult American men are at least six feet tall).
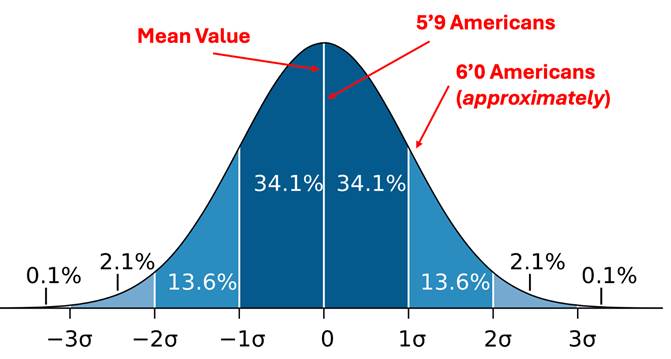
Sensitivity to pharmaceuticals and environmental toxins (e.g., synthetic chemicals) follows a similar pattern, with a minority of the population existing which is extremely sensitive to these things (and conversely, on the end of the bell curve, another minority exists on the opposite end which has a very high tolerance to them).
I’ve always felt genuinely bad for the class of sensitive people as the medical system frequently dismisses their symptoms (as the majority of patients do not share their sensitivities) and they are often left along to struggle with a variety of things most people can’t relate to, yet along [let alone?] empathize with.
Note: I’ve tried to use Substack to bring attention to their situation (e.g.,
1. this article discusses the unique sensitivities patients in this constitutional archetype experience,
2. this article explains the frequent associate between ligamentous laxity and pharmaceutical injuries along with how things like manganese can be used to treat hypermobility and
3. this article reviews the dysfunctional mitochondrial danger response many of them are stuck in).
For additional context, I consider myself a “somewhat environmentally sensitive” individual, but I have been close to numerous “highly sensitive” individuals and witnessed what they go through each day firsthand.
One of
the major challenge with all of the environmental toxins we are exposed to is
determining how much our exposures to each of them actually matters, as there
are so many of them it borders on impossible to identify which ones are
actually directly responsible for the chronic illness an individual
experiences. That said, a few individuals like Joseph Pizzorno have
done a remarkable job of quantifying the evidence that demonstrates the harms
these toxins have created, and in clinical practice, we periodically see a
complex and debilitating illness resolve once a comprehensive detoxification
protocol is administered which addresses toxin exposures that occurred years if
not decades ago.
Note: in a recent article I
shared our observations which substantiate that a massive decline in the
health of the human species has occurred over the last 200 years and listed
what I presently believe to be the key culprits.
The highly sensitive individuals frequently refer to themselves as “canaries” under the logic that the same environmental toxins they experience severe reactions to are also affecting everyone else on a more subtle and insidious way (e.g., by giving them cancer ten years down the road). I’ve taken this point to heart, and both used them as an early warning sign something is dangerous and a guidepost for all the things in the environment I should be avoiding, under the logic that if I mostly avoid all the things the canaries are sensitive to, I probably won’t have any major health issues (which has so far held true).
The COVID
vaccines in turn help to illustrate many of these concepts. For
instance, since they are a highly toxic agent, immediately once they hit the
market, I began to have numerous patients show
up who had severe reactions to them (which suggested their average injury value
was very high) and hence was not surprised as I began to hear more and more
stories of sudden death following their use, and later numerous insidious
chronic complications of the shots that onset in the years after the injection.
Likewise, while I was hearing all of those injury reports (which I
compiled here), I noticed
within them there was also a smaller number of unvaccinated
individuals who were developing similar symptoms (e.g., menstrual
abnormalities) after spending time with someone who had been recently
vaccinated. This prompted me to begin reaching out to the sensitive individuals
I knew (along with looking for online reports such as the video I included in this article).
Once I found a few sensitive individuals who could immediately tell if someone had been vaccinated from [merely] being around them,
1) I concluded shedding was a very real thing and
2) began looking for a way to explain it (as mechanistically it seemed impossible the mRNA vaccines could shed).
Since that time, those mechanisms have been identified, and through working with Pierre Kory (who has many patients whose labs show they are affected by shedding) I’ve collected over 1,000 reports of shedding injuries which occurred in a fairly consistent and reproducible manner (and likewise could be treated in a fairly repeatable manner).
Clothing Toxicity
One of the frequent points I raise here is that our regulation of pharmaceuticals drugs is woefully inaccurate due to there being so much money in medicine there is inevitably enough to pay off a bureaucrat to approve and then often mandate dangerous and ineffective products (e.g., all the data showed Paxlovid was useless but the government nonetheless spent billions giving it to America).
However,
while the pharmaceutical situation is abysmal, it’s actually much better than
the cosmetic industry, as very few resources are devoted towards ensuring those
products are safe. In turn, I’ve lost count of how many people I’ve met who
discovered they reacted to specific chemicals in their shampoo, makeup or soaps and were forced to gradually shift to
all natural products to get through life. In turn, I avoid most of the products
on the market and try to either make the ones I use at home (as that way I can
guarantee what’s in them) or buy very specific brands we believe are clean.
Note: as many natural skin
care products contain biological proteins in them, every once in a while I come across a case of someone who developed an
allergic reaction to a natural product. Fortunately this is quite rare.
Sadly, while some regulation exists for cosmetics, almost none exists for fabrics or the chemicals put onto them (other than things like mattresses needing flame retardants—many of which are toxic). Because of this, we wear a lot of things we just should not be wearing.
With clothing, because of how I react to synthetic fabrics like polyester (they just don’t feel good on me—for example when it’s hot and I sweat it often feels as through plastic fibers are coming into my skin), I’ve long suspected they are significant issues with the fabrics. Likewise, the tendency for feet to sweat is why I believe having socks made from a natural (and relatively dye free fabric) is fairly important.
Note: one of the most intriguing models I’ve come across to explain why synthetic clothing causes issues arises from the fact that unlike natural fabrics, they generate positive ions around the wearer, which I believe is due to them removing negative charges from the surfaces they contact (which for reference is the mechanism behind static electricity). Excessive positive ions (or a lack of negative ions) in turn have been linked to a variety of health conditions, many of which I believe are reflective of them weakening the (negative) physiologic zeta potential in their immediate vicinity (e.g., most of the existing data demonstrates their adverse effect the respiratory tract which makes sense since positive ion exposure is typically through inhalation). In certain cases, the skin is also extremely responsive to changes to zeta potential (e.g., much of the data on negative ion therapy was gathered from burn units—a challenging illness condition known to be heavily influenced by blood sludging [which in turn results from impaired zeta potential]), so the positive ion from synthetic fabrics may be account for some of the reactions these fabrics cause.
Since a few of my colleagues have had similar experiences with clothing, we’ve made a point over the years to ask our highly sensitive patients how they respond to clothes and have found the following:
•Quite
a few of them learn on their own that they need to wash new clothes before
buying them. Furthermore, some find they need to wash them 3 or so times before
they can wear them without reacting to the clothing. Additionally, they must
almost always use a clean and fragrance free detergent, and one of my own
struggles is to make sure my clothes never get cleaned in a toxic detergent
because the smell will often linger with the clothes for a long time.
Note: more sensitive patients
have difficulty being in large stores that have a detergent section, because
even while sealed, they still emit an odor which can be smelled from quite far
away. Likewise, I’ve heard of cases where they had to move out of their house
because someone used a typical detergent in the house’s laundry machines and of
them having difficulties being around people wearing clothes which had been
cleaned in a typical detergent.
•Reactivities to synthetic fabrics is quite common.
•The option to buy organic fabric exists
(e.g., clothes made from organic cotton). Given how cotton is produced, I
thought that this would be important but it comes up fairly rarely and
typically only in cases where they have prolonged exposure to the fabric (e.g.,
we had a patient who we eventually discovered needed to sleep on organic bed
sheets to stop the significant symptoms they were being plagued by).
Note: a certain subset of
sensitive patients have issues with the dyes often used in clothing and I
suspect they have a greater need for organic clothing.
•Many
of them find they cannot tolerate the labels
on their clothes (e.g., the one at the top of the back of most t-shirts)
contacting their skin and have to cut it off.
Note: We are still not sure if
this is reaction is chemical or physical (from it rubbing against this skin) or
both.
•Many
of the reactions our sensitive patients exhibit resemble mass cell reactions.
Note: mast cell disorders are
frequently seen in the sensitive patient population and are one of the most
common chronic spike protein injuries. In this article, I discuss how mast cell disorders are
often linked to blood stagnation.
Additionally, I’ve also met numerous people who react to scented products others are wearing (e.g., colognes, body sprays, or perfume), but sadly the wearers rarely consider how that choice will affect their target audience.
Clothing Fitting
While the fabrics you use matter, I presently believe how they fit to your body is more important as tightly fitting clothes (or rings) can restrict many important circulations through the body. In turn, we frequently notice sensitive patients with chronic illnesses of their own volition will chose to wear looser and looser clothes—something I believe is due to those patients frequently having an already impaired fluid circulation throughout their body (as complex illnesses often go hand in hand with an impaired zeta potential and as mentioned above, easily compressible vessels).
I will now focus on four specific areas.
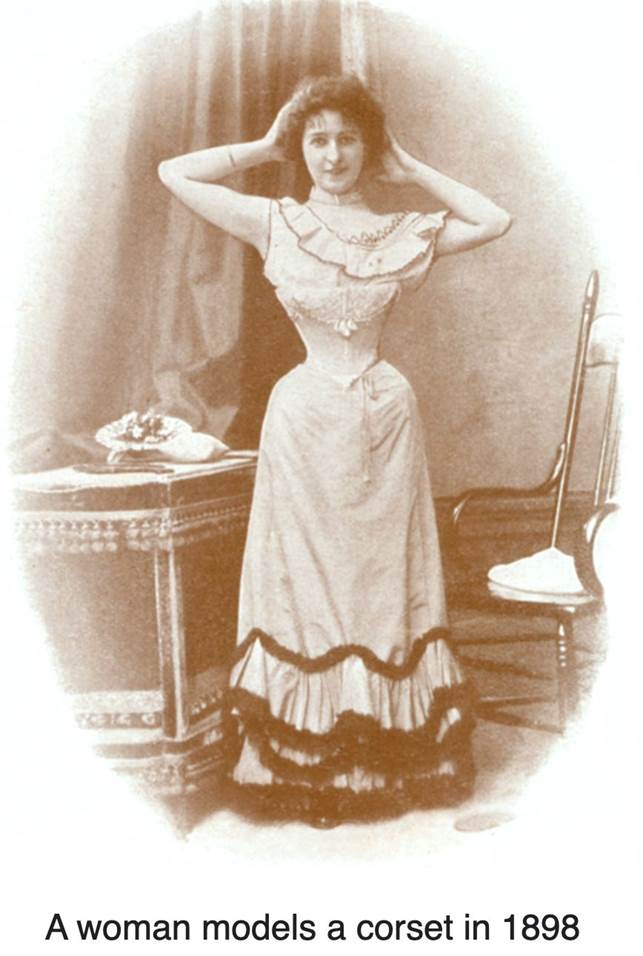
Corsets
Something most men have difficulty appreciating (yet alone empathizing with) is how much pressure society (e.g., in America) places women under to conform to specific appearances that largely exist to fund the fashion industry. The worst of these offenders were the corsets, which to quote Wikipedia were:
A corset is a support undergarment worn to hold and train the torso into the desired shape and posture. They are traditionally constructed out of fabric with boning made of whalebone or steel, a stiff panel in the front called a busk which holds the torso rigidly upright, and some form of lacing which allows the garment to be tightened. Corsets were an essential undergarment in European women's fashion from the 17th century to the early 20th century. In the 17th and 18th centuries they were commonly known as "stays" and had a more conical shape. This later evolved into the curvaceous 19th century form which is commonly associated with the corset today. By the beginning of the 20th century, shifting gender roles and the onsets of World War I and II (and the associated material shortages) led the corset to be largely discarded by mainstream fashion. As you might imagine, wearing that was not the best thing for one’s health:
As you might imagine, wearing that was not the best thing for one’s health:
While not usually deadly, wearing a tightly laced corset can be quite harmful to the wearer. They can reduce lung capacity, cause shortness of breath and fainting, produce skin irritations, compress the ribs, weaken back and chest muscles and have even been known to cause organ deformity. Tight corsetry can also exacerbate lung conditions such as pneumonia, dangerously restrict digestion, cause constipation and can also worsen any existing issues within a woman’s reproductive system. Remarkably enough, a “maternity corset” was designed in the 1830s, allowing pregnant women to stay in fashion. Despite the spatial allowance made by the corset maker, however, it still caused great harm to both mother and child.
While it seems absurd people would do that, we still have many vestiges of it today. For instance, women are often encouraged to compress their waist and breathe through their chest to attain the elusive hourglass figure (which is not healthy), and numerous breathing instructors have shared that one of the greatest challenges they’ve faced in teaching abdominal breathing (which is great for your health) is that the women they teach often have a great deal of difficulty doing something that goes against their conditioning to have a thin waist. Likewise, many less extreme corsets (e.g., the “waist trainers”) are commonly sold online because a lot of people buy them.
Bras
Note: this section is a bit longer but provides context for things that follow which are directly relevant to men.
Presently, Americans spend roughly 20 billion dollars a year on bras, which is remarkable given that prior to a century ago (the 1910s to be precise), almost no one wore them (whereas now between 80-90% of women do). In turn, almost every women assumes bras are something women have always worn and are not aware of the massive marketing campaign the fashion industry did to normalize this practice (which was essentially done as a pivot because they could no longer sell corsets to women).
Since women never wore bras for most of human history, it raises a simple question—might there be any downsides to the practice?
Presently, I believe a good case can be made for the following:
Pain—bras
frequently cause chronic back or rib pain (which goes hand in hand with
restricted breathing) along with neck, shoulder and breast pain, and as many
women can attest, it feels so good to take your bra off. In turn, whenever I
have a patient who complains about pain in the region of her back or rib that
her bra digs into, I counsel them to consider removing the bra.
What is remarkable about this is that most women recognize this (e.g., a survey of 3000 women found
that 46% of them enjoy being able to take their bras off at the end of the day,
while another 3000 women survey found
52% take it off within 30 minutes of getting home) and during the pandemic many
women stated they stopped wearing a bra once
the lockdowns allowed them to work from home and hence not “need” one.
Likewise, when 3000 women were asked to characterize their bras, 21% selected
“An Enemy – I wish I had never met her,” 14% chose "A Business Partner – I
put up with her" and “uncomfortable” was the most common word women shared
to describe their bra.
Nonetheless, most women still wear them in public (which I feel helps to
illustrate how unfair many things in our society can be—e.g., women that object
to subjecting themselves to this are often trivialized as irrational “bra
burning feminists”).
Note: a case can be made that
many of these issues result from improperly fitted bras. However, given that
every report finds the majority of women have “improperly fitted bras” (often
citing an 80% figure) and this issue has been known about for years, I do not
believe this is something that will ever be addressed with “better fitting.”
Breast Shape—one of the most controversial points on this subject is if wearing a bra “worsens” the shape and quality of one’s breasts. Very limited evidence exists to support this contention (e.g., that it increases sagging overtime), but the honest truth is that no one has ever wanted to formally study this in a large trial, so it’s technically “unproven.” That said, in my own observation (and that of others like this gynecologist) is that not wearing a bra is cosmetically beneficial to the breasts. I mention this because one of the most common marketing tropes for bras is that they help one maintain the breast’s youthful appearence.
Metal Allergies—One estimate found 17% of women are allergic to nickel (whereas 3% of men are) and hence suffer issues where it contacts the skin. This is frequently a problem for bras because their underwire is normally made from nickel (due to it being the cheapest material to use) and the nickel frequently coming in contact with the skin (due to sweat leaching it out and friction rubbing it against the skin). Remarkably, despite many women being sensitive to nickel bras, the industry has not been motivated to make nickel free ones be easily accessible to women (which is something I’ve always found extraordinary).
Note: a variety of other products (e.g., buttons, glasses, and belts) also use nickel, so a potential nickel allergy is always something that should be considered when unusual symptoms start, particularly in a localized area. For those interested in learning more about nickel allergies, this article describes a lot of it from a patient’s perspective.
Impaired
Circulation—since the bras compress the breast, it’s reasonable that they might
also impair their circulation and numerous anecdotal reports support this.
Likewise, this may explain some of the other issues commonly associated with
bras (e.g., headaches and indigestion). However, in my opinion, the greatest
issue is impaired lymphatic drainage from the breasts (as lymphatic
circulation is very sensitive to being obstructed by an external pressure).
Note: this Venezuelan study (which you have to translate) is
an example of a study that found bras created a variety of issues for the
breasts and that the rate of these issues increased as they were worn more
frequently.
Breast
Cancer—the most taboo subject with bras is their link to breast cancer, and as
in turn, every
major cancer organization attacks this contention, insisting there is no
evidence to support it. Conversely, an argument can be made it is plausible since many
holistic schools of medicine have found cancers are linked to lymphatic
stagnation and the most common site of breast cancer (the upper outer quadrant which
lies before the armpits) is also a primary lymphatic drainage site
for the breasts. Furthermore, there are some
conventional sources that support this assertion (e.g., this article from
a Dermatology journal highlights how many skin cancers are associated with
regions of lymphatic stasis and cites evidence indicating that is a product of
lymphatic stasis creating immune stasis that promotes tumor growth). Likewise,
there is some acknowledgment within mainstream sources that
bras create lymphatic stasis which can give rise to breast cysts.
Note: in addition to the
lymphatic stagnation hypothesis, some also believe bras with metals may
function as antennas that concentrate carcinogenic EMFs at the breasts, but I am not aware of any research that has
formally evaluated this. Additionally, people have suspected aluminum
(which is contained in deodorants and antiperspirants) may be linked to breast
cancer as it is frequently found in cancerous breast tissue (and likely being trapped by there by the lymphatic
obstruction created by bra wearing). The
scientific community has vehemently denied the link between these aluminum
products and breast cancer, but in recent years, some evidence has accumulated
to support this
contention. I find this link noteworthy, as due to its adverse effects on zeta potential, aluminum is one of the most effective
agents that exists for creating lymphatic obstruction.
In
turn, there is some evidence to support the contention bras are linked to
breast cancer. Specifically:
•A 1991 Harvard
study of 9333 people found “Premenopausal women who
do not wear bras had half the risk of breast cancer compared with bra users.”
•A 1991-93 study of
5000 women that found:
· Women who wore their bras 24 hours per day had a 3 out of 4 chance of developing breast cancer.
· Women who wore their bras for more than 12 hours but not to bed had a 1 in 7 risk for breast cancer.
· Wearing a bra less than 12 hours per day dropped breast cancer risk to 1 in 152.
· Women who never or rarely wore bras had a 1 in 168 risk for breast cancer.
This for
reference is 4-8 stronger than the association between smoking and lung cancer
and is discussed further in the book Dressed To Kill: The Link Between
Breast Cancer.
Note: the authors did
a followup study in 2000 in Fiji (where half of women don’t wear bras) and were
able to identify 24 cases of breast cancer, all of which they then found
occurred in women who had worn bras (whereas no cancers were found in the women
in their village who did not wear bras). Additionally, they also published an article describing
the mechanisms they believe underlie bras causing breast cancer.
•A 2009 Chinese study found that avoiding sleeping in a bra lowered the risk of breast cancer by 60%.
•A 2012 Chinese study of
400 women found sleeping with a bra made women 1.9 times more likely to develop
breast cancer.
•A 2015 Keyan study of
694 women found wearing a bra all the time (including while sleeping) made them
3.4 times more likely to develop breast cancer.
•2016 Brazilian study of
304 women found women who were frequent bra wearers had were 2.27 times more
likes [likely] to have breast cancer.
•A 2016 meta analysis comprised
of 12 studies found wearing a bra while sleeping doubled one’s risk of breast
cancer.
Note: this is one of the most detailed papers on this subject, so I would
advise reading it if you are seriously interested in the topic.
•A 2019 Iranian study of 360 women found women with breast cancer on average wore bras longer than women without, with the greatest being observed in how long it was worn while the slept. The increased risks of breast cancer seen here were smaller than those in the other studies but still were statistically significant.
•Conversely,
there is also one 2014 study (produced
by researchers at a major cancer center that takes in a lot of corporate money
to bring new cancer pharmaceuticals to market)
which refutes the link between bras and breast cancer. This study is repeatedly cited by establishment cancer organizations to
debunk the link between the two, and in many cases, those organizations also
falsely claim it is the only scientific study that ever
evaluated the link between bras and breast cancer. Critics of this
study, in turn, suspect it’s negative finding were in part due to it only
evaluating post menopausal women whereas the previous studies found the
association in premenopausal women.
Note: I am somewhat skeptical of this study because it is extremely common
for the medical industrial complex to first ignore or ridicule mountains of
data which threaten its financial interests and then
eventually have an establishment site conduct a study which was designed to get
a negative result (e.g., by deliberately administering the treatment too late
in the disease process) and then trumpeting that study as proof all the other
studies were a hoax. This for example happened to the alternative cancer
treatment laetrile, IV vitamin C for sepsis,
and both hydroxychoroquine and ivermectin throughout
COVID-19.
In turn,
my feelings on this subject are as follows:
•You should try going without a bra and see how it makes you feel. If you feel
better, you should ask why you are forcing yourself to wear one (and spend
quite a bit of money on them).
•If you decide to go without a bra, there are a variety of approaches you can
do which conceal that from outside observers (e.g., by wearing thicker and
looser fabrics).
•Some women (e.g., those with large breasts) do need bras for support. However,
I do not believe this applies to the majority of women.
•If you wear a bra, it should be appropriately fitted (which can be
surprisingly challenging to do) and it should not have an underwire.
•If you wear a bra, you should minimize the amount of time you do it, and under no
circumstances do so when you sleep.
•If you have a daughter, you should encourage them not to wear training bras
(which the fashion industry has somehow managed to be a ritual into womanhood
for many of our children).
Ties
Ever
since I was young, neckties have never been something I could relate to (e.g.,
one of my first memories of them was associating them with Mr. Snuffleupagus from
Sesame Street and thinking it was weird people would want to have an elephant
trunk hang off them). As I entered practice, I began to notice I would
periodically see patients who appeared to be developing symptoms from the tie
impeding blood flow in or out of their neck due to it being tied too tightly.
This in turn prompted me to ask why they had tied it so tightly, at which point
I learned it is quite difficult to make a tie look nice without it also being
moderately tight.
Note: my present solution here
is to recommend wearing a bow tie instead as they do not need to be as tight to
consistently look nice.
There
is also some data to support my observations. For example:
•A 2003 study found
that wearing a tie increased the interocular pressure within the eyes, leading
to the authors suspecting ties may also be tied to glaucoma.
•A 2011 study found
neckties decreased cerebrovascular reactivity (the ability of cerebral vessels
to dilate or constrict in response to challenges or maneuvers), which suggests
it also impaired cerebral blood flow.
•A 2018 MRI study
found wearing a tie decreased blood flow to the head by 5.7%.
Note: since ties often are colonized by bacteria, they are frequently cited as a potential vector for doctors transmitting infectious diseases to patients. Presently, it’s unclear if sufficient evidence exists to support that contention.
Pants
Another unfortunate fashion trend is wearing tight pants. As I hope the above points show, this can be potentially problematic, and we periodically see patients who are suffering from pants that are just too tight.
Some
of the common issues with tight pants include:
•Impaired blood or lymphatic flow too and from the legs (which is particularly
easy to disrupt in chronically ill patients like the hypermobile ones mentioned
above). Once this blood flow is disrupted, it can in turn lead to a variety of
issues such as numbness, tingling, coldness or weakness in the legs.
Note: some of these
issues have also been observed in COVID-19
vaccine injured patients due to them having a variant of
May-Thurner syndrome.
•Becoming twice as likely to
develop severe pain in the vulva region (termed vulvodynia), along with other
forms of irritation from the tight pants rubbing against the area.
Additionally, many believe tight
pants can also cause microbial imbalances of the vagina (e.g., bacterial
vaginosis).
•Testicular compression, which many believe can reduce the male sperm count
(since it is heat sensitive) or cause testicular cancer. As best as I can tell,
very little research exists on either of these (but some does—e.g., numerous studies show
looser underpants increases one’s sperm count while this study showed
tight fitting underwear and pants made a man 2.5 times more likely to have
impaired semen quality).
•A 2012 survey of
2000 men wearing skinny jeans found 50% experienced groin discomfort, more than
25% suffered bladder problems, and 1 in 5 men experienced a twisted testicle.
Note: men are likely more
sensitive to tight jeans due to their external genitalia.
•Significant numbness, tingling, and pain (e.g., burning) in the outer lateral thigh due to tight pants compressing the lateral femoral cutaneous nerve.
Note: there are a variety of other condition tight jeans are thought to be linked to (e.g., acid reflex or a hiatal hernia) but the data again is much less clear.
Additionally, since arterial, lymphatic and venous circulation to the legs is frequently quite important, I believe this accounts for why chronically ill patients (who already have compromised fluid circulations in their body) are frequently compelled to start wearing loose pants, and in this instance, they again represent the “canaries in the coal mine” who are warning us against the harms of tight clothing.
Trusting Your Body
One of the major problems we face in life is determining how to make decisions in the face of uncertain information, especially since the funding we rely upon to create our scientific knowledge tends to be biased to arrive at conclusions that make money, not ones that promote health. In turn, as I highlighted in this article, there are a lot of simple things with clothing you would have thought would have been exhaustively studied but never actually have been (whereas I showed in the last article, we frequently spend millions of dollars conducting completely unneeded and inhumane animal experiments).
Because
of this, I often find we have to rely on
alternative ways of knowing, and one of the most reliable (but
frequently dismissed ones) is listening to our bodies, which for instance is
what actually drove me to adopt the wardrobe I utilize, and similarly drove
many of the chronically ill patients I mentioned above to do the same. My hope
in turn by writing this article is to encourage you to chose clothes on the
basis of how they feel, not how they look.
Note: last year I published
a detailed article about what constitutes the optimal
diet where I essentially argued that while there are some foods everyone should
avoid (e.g., most processed foods) because there is so much variability in
metabolic types from person to person, no “ideal” diet exists and evidence can
be found to support every one of them depending on which subset of people you
evaluated. In that article, I thus stated the key to a healthy diet is to be
able to listen to your body and know how to make sense of what it is telling
you as I felt that provided the necessary context for the second part of the series (our preferred approaches for weight
loss).
Sadly, our society has done an incredibly effective job in convincing us to not listen to their own intuition so we will continue to be compliant customers. For instance, I’ve lost count of how many heartbreaking pharmaceutical injury stories I’ve heard where the patient stated they felt apprehensive about taking the drug or vaccine, eventually agreed to take it because the doctor badgered them into it, then continued doing so once they experienced severe side effects (which their doctor told them didn’t matter), and that once they became permanently disabled, their greatest regret was not listening to their body and their intuition. One of the main reasons I cited the bra example was to illustrate that despite bras being a modern creation and around half of women stating they do not like wearing them, because of how much money is behind that industry, it’s managed to reshape our society so that most women still do.
In the final part of this month’s open thread, I will touch upon the types of clothing we currently endorse wearing (which was the product of years of investigation), and the cosmetic products (e.g., detergents for clothes, soaps and toothpastes) we have found are the least toxic, along with reviewing a few of the more taboo subjects this article touched upon (e.g., how everything mentioned here relates to some of the more concerning practices transgendered youth are now being encouraged to do).
Breast Binding and Tucking
Many of the transgendered youth who yearn for gender reassignment surgeries aren’t able to get them (e.g., due to cost or obtaining permission for one). In turn, a “compromise” which is often proposed to them is to wear tight clothing which conceals their “undesirable” body parts.
This
is accomplished either through wearing a tight wrap around the chest which
compresses and flattens the breasts (known as breast binding),
or pushing the testicles back into their canal and compressing the penis (known
as tucking).
While this seems unbelievable (and hopefully as this article showed unsafe), I
want to emphasize that there are actually a lot of people doing it and it’s
very easy to find how to guides online encouraging you to do it.
As both these practices haven’t really been studied, their risks are somewhat unknown.
In the case of tucking, some of the risks thought to be associated with the
practice include:
•Chafing and discomfort
•Urinary tract infections
•Problems with urine flow
•Twisting or inflammation in the testicles
•Increased body temperature of the testes, which can affect fertility
•Premature death of sperm inside the testicles, leading to lower sperm count
•Testicular torsions.
I also suspect tucking may become linked to testicular cancer as an undescended
testicle has long been known to be one of the greatest risk factors for
testicular cancer.
In
the case of breast binding, some of the suspected risks of it (which overlap
with the dangers of wearing corsets) include:
•Chest pain
•Scarring
•Overheating
•Shortness of breath
•A buildup of fluid in the lungs
•Difficulty breathing
•Backache
•Skin rashes
•Rib deformities
•Permanent damage to the elasticity of the breast.
I
find the breast finding fad quite sad as it builds on a long history of
misogynistic practices. Beyond corsets, binding has been used throughout
history to prevent women from looking “lewd” or
attracting the sexual attention of men (especially in more oppressive societies
where women lacked basic rights like imperial china or Irish asylums where
thousands of “immoral” women were forced to live in the not too distant past)
and there have been numerous times where American fashion has encouraged women
to breast bind so that their femininity will not get in the way of what they
are supposed to be doing (e.g., office work).
Furthermore, many societies go further than just breast binding. For instance:
Breast ironing, also known as breast flattening, is the pounding and massaging of a pubescent girl's breasts, using hard or heated objects, to try to make them stop developing or disappear.
This practice in turn is rationalized under the idea that it protects the girls from being sexually targeted by men who may impregnate or infect her (e.g., with HIV).
I hence find it remarkable that despite this practice being widely condemned, our culture is simultaneously both encouraging breast binding of our children and the more extreme version of breast ironing (highly lucrative surgical removals of the breasts), particularly given that a political climate has been created where one is likely to be attacked for so much as questioning the safety of the practice.
Note: a variety of other unscrupulous clothing practices also periodically emerge throughout history. For example, imperial china was well known for the practice of foot binding, where women’s feet would be broken and then tightly wrapped so that they developed a more feminine figure (as the deformed feet were deemed “attractive”). This practice understandably caused a lot of problems (e.g., it was very painful and could result in lifelong disability) but nonetheless it persisted for centuries and in the early 19th century, it was estimated that 40-50% of Chinese women and almost all upper class Han Chinese women had been subjected to this procedure. I share this to again illustrate how society’s (especially once money is involved) can easily become fixated on the need to perform an invasive modification to the body which in hindsight looks abhorrent. Additionally, I’ve never liked high heels and found it quite noteworthy that they create similar (but far less extreme) changes in the feet to that accomplished by foot binding.

Home Products
There is a wonderful organization called the Environmental Working Group which evaluates almost all of the cleaning and cosmetic products on the market (along with many other things like produce) and offers insight into which ones are the safest. Many chemically sensitive individuals in turn find this group invaluable for determining which products they should use.
Years ago, I consulted the EWG to determine which detergent was the cleanest and found they endorsed the ECOS brand, which conveniently was sold at Costco (where it cost around a quarter of what it did in health food stores) and since it felt fine, I never stopped using it. In turn, over the years, I found many of my colleagues also shifted towards using it and we’ve all found the fragrance free one rarely created issues for our patients. While writing this article, I checked the EWG’s current list and discovered that they have since found even cleaner laundry detergents, and no longer give the highest rating to ECOS. For this reason, I still endorse ECOS, but believe those who are particularly concerned about this issue should consider using the EWG’s guide to identify a cleaner product that is available in their stores.
In the case of soaps, I’ve long been a fan of Dr. Bronner’s products since I believe the company has a good ethos it operates from, their ingredients are fairly clean (e.g., EWG gives their second highest rating to their liquid soaps and their highest rating to the solid soaps) and because a single one of their soap products (especially the liquid ones) are affordable, easy to find and last for a long time. However, I don’t believe it’s a perfect solution because our more sensitive patients have reacted to the liquid Bronner formulations and hence needed a cleaner and less “harsh” soap product. This for example is why the EWG lists can often be extremely helpful.
A
variety of other household products also exist which I’ve followed a similar
process with (e.g., I find it’s important to use green cleaning supplies in the
house and I never stay in places that use air fresheners). As that encapsulates
a fairly long list of products I won’t list most of them but did want to
mention:
•Spry makes
the cleanest toothpaste and mouthwash we’ve found (which sometimes is quite
helpful such as for patients experiencing inexplicable facial allergies resulting
from their dental products).
•Organic coconut oil often can function
as a replacement for hair products (e.g., conditioner).
•White vinegar can sometimes serve as a substitute for the products you would normally use to clean your house.
Natural Fabrics
A
variety of natural and synthetic fabrics exists. As mentioned before, generally
speaking, I greatly prefer natural fabrics (e.g., because they don’t create
positive ions). Most commonly, the following
options for natural fabrics exist:
•Bamboo
•Cotton
•Hemp
•Linen (which is made from flax).
•Silk
•Wool
In turn, pros and cons of each exist. My thoughts on each are as follows:
Bamboo—a lot of people aren’t aware this option exists and sensitive patients
often do quite well on it.
Cotton—this is typically the easiest natural fabric to find high quality dress
clothes in. As a result, it’s often necessary to use, and typically does not
provoke reactions in those who wear it.
Hemp—this has always been one of my favorite fabrics due to how it feels and
its durability. Due to the taboos against hemp, until recently it was difficult
to get the right hemp clothing, but now that its production is increasing,
decent hemp clothing options are becoming easier to find.
Linen—this fabric also feels nice, but unlike hemp is much easier to find. For
this reason, I’ve ordered numerous linen clothing products over the year when I
could not find a hemp equivalent.
Silk—silk is quite comfortable but is expensive and requires significant care
(e.g., it can be damaged in the wash). While some people find that hassle is
worth the benefits of wearing silk clothing, I personally believe the best use
for them are for bed sheets (as some people really like sleeping on silk bed
sheets and they rarely cause health issues).
•Wood—wool varies immense depending on its quality (high quality wool feels
amazing but expensive, while sensitive patients often can’t tolerate the more
generic wools) and it is often a lot of work to properly maintain (since it
can’t tolerate being put through a normal washing machine). In addition to
looking nice, I believe one of the biggest (but relatively unrecognized) uses
of it is to wear a wool t-shirt at night if you sweat frequently because the
wool can make night sweats much more tolerable (e.g., one patient told me it
was life changing once they figured it out).
Note: when I was writing this article, I went back and forth on endorsing a specific bra as there are some which are dramatically more comfortable, but I simultaneously don’t want to be supporting the industry in any manner. For this reason, I won’t list a specific one, but I will mention one less appreciated option is that for social functions where a bra is needed, you can wear silicon nipple coverings which provide the appearance that you are indeed wearing a bra.
Conclusion
Since I like to review written texts from the past, I often wonder what the logical basis was for many of the customs ancient cultures had we now see as simple superstitions (e.g., I believe there was a medical basis behind prohibiting some of the foods older religions did not permit their followers to eat).
In exploring this subject, a Jewish custom, known as Shatnez came to mind, which is based on two verses from the old testament (this one and this one) which state that you should not wear garments made of two different types of material, specifically focusing on wool and linen being woven together. In turn, due to Jewish law prohibiting wearing mixed fabrics, a lot of work has gone into finding ways to determine if clothes are indeed “adulterated” and made from different linens (as in every era counter fitting is quite common—e.g., the current olive oil situation is quite depressing).
Like many things in the ancient religious texts, a lot of different theories exist for why these verses ended up in the old testament (e.g., it may have been entirely political, economic or done to help promote animal welfare). Nonetheless, to me it suggests some members of society have always been aware of the effects your garments can have upon you (and in turn I can see a variety of possibilities for why mixed fabrics might have created issues).
I hope that this article opened you up to the forgotten side of clothing and provided some useful insights you may be able to apply to your life. I sincerely thank each of you for your support of this publication and making the work I am doing here (and outside of Substack for the world) possible.